
After last week’s whiny post about how I’ve been so disappointed in my diabetes devices lately, I feel compelled to let the pendulum swing in the other direction and give credit where credit is due.
About a week and a half ago, Dexcom rolled out its G5 Mobile app to Android users. Finally. Okay, I said I would give credit where credit is due. And kudos to Dexcom, who, as far as I can tell, is the only device maker to develop software to use on an Android platform. Yay!
I know all of you iPhone Dexcom users are yawning right now, but please give me a moment to be happy too. I’m a person who can appreciate the wonders of a good smart phone, but I can’t bring myself to pay hundreds of extra dollars because there’s an image of an apple on it. After years (literally, years) of waiting for an Android option, Dexcom has come through.

Among other things, this means no more carrying around the receiver. I’m a guy who carries too much in my pockets already. I do not need one more thing to lug around, and even though the receiver wasn’t too big, not having to carry it around feels like a big weight off of my… pockets.
In addition, I’ve finally completed my Clarity account setup, which means my endocrinologist can get my Dex data too. No more downloading the data at the office visit. She’ll have it already. Cool, huh?
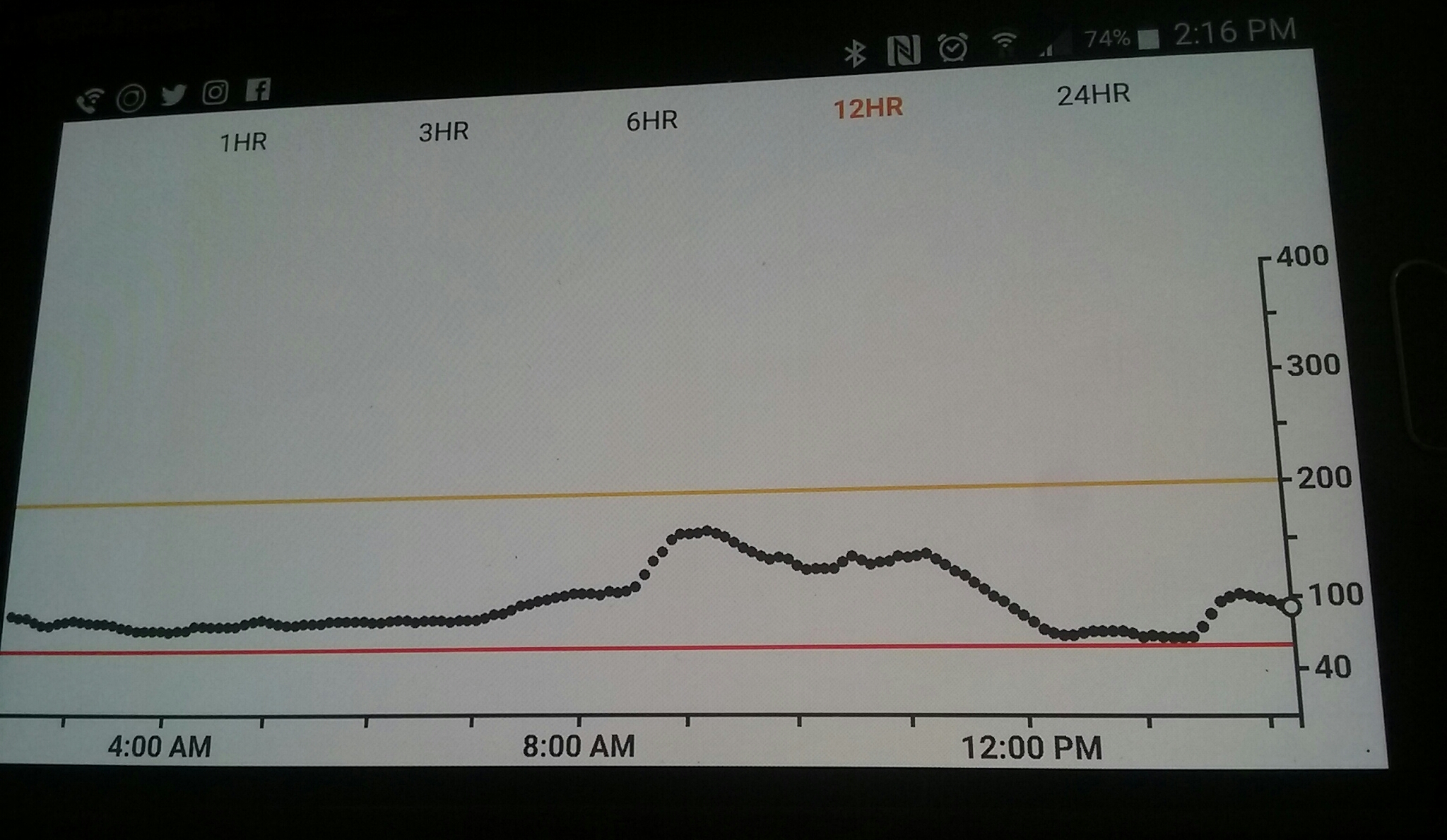
I’m getting the hang of navigating the G5 Mobile app. It took me a couple of days to realize that I needed to turn the phone to landscape view to be able to see more than the last three hours’ worth of data. Once I do, it’s just a push of a button to view my data in 1 hour, 3 hour, 6 hour, 12 hour, or 24 hour increments. If I hover my finger at any point in the graph, it will show what my reading was at that very point.
And I have to admit to having a little fun with the alert sounds. Instead of the basic Vibrate, soft, attentive, etc. settings available on the receiver, I have 23 different sounds to choose from. So if I want to have my low alert set to Truck Siren or Blamo Dings, I can do that. Nice touch.

I get that making an app work on two different platforms is extra work, but I am SO HAPPY that Dexcom has made the effort. Reducing the burden of managing diabetes is a good thing, and to that extent, Dexcom has done it.
The Dexcom G5 Mobile app for Android users is available for free in the Google Play store right now.
My apologies for the off-center views of my phone screen. Security features built into the app will not allow for a screen capture, so I had to take photos of my phone screen.
Disclosure: I was not given anything or asked to write anything about the Dexcom G5 Mobile app. All opinions are, as always, my own.




