Every now and then, I look back and realize just how far we’ve come in less than ten years. I realize access is an issue, and it deserves its place and time. But for this moment in time, I’d like to focus on the sheer magnitude of advances we’ve witnessed over the last decade.
Part of the story of the birth of this blog comes from a radio interview heard by The Great Spousal Unit one day. She called me at work, very excited, and told me I needed to listen to it with her after work that night.
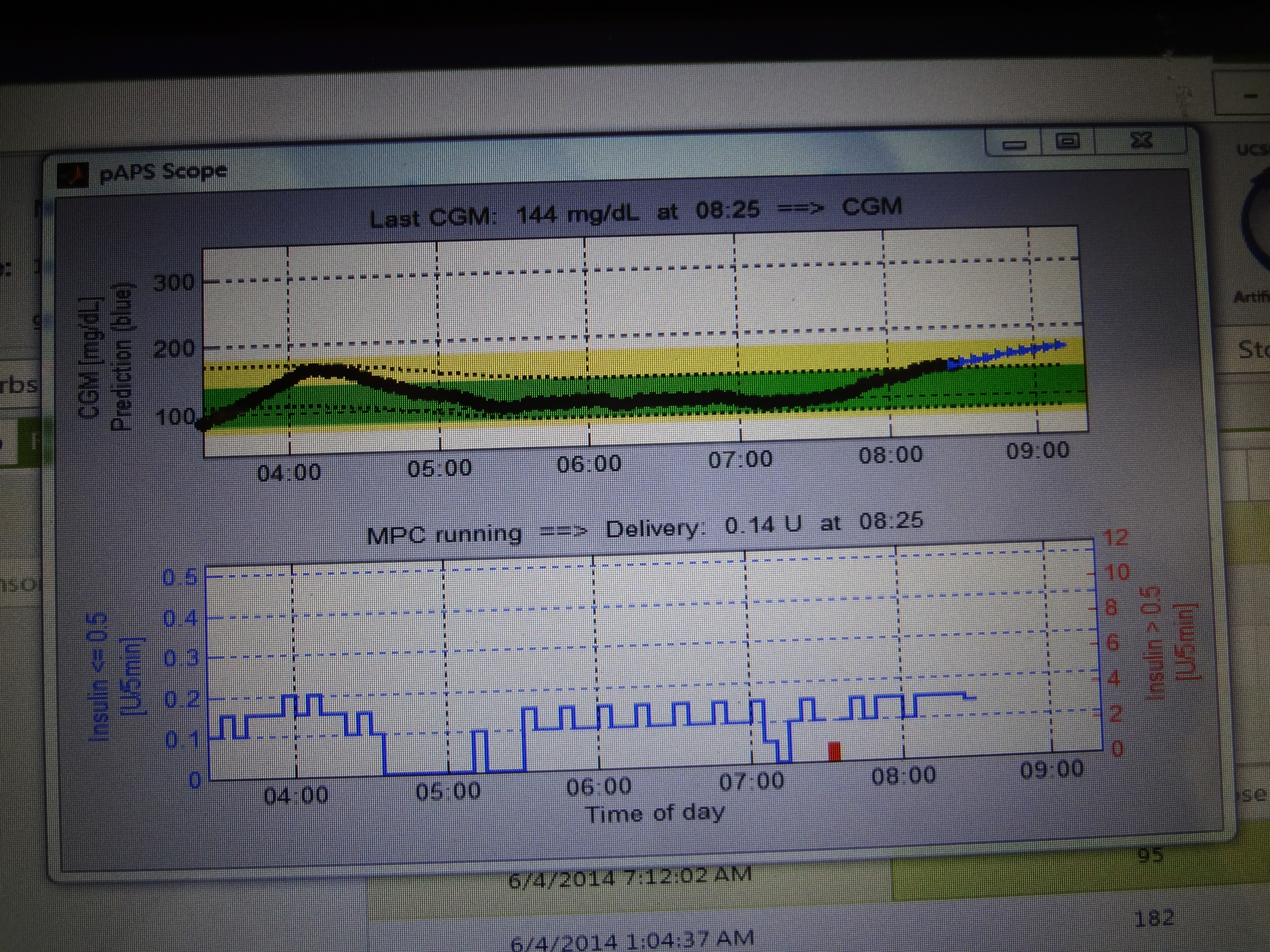
The interview was about artificial pancreas technology. The year was 2011.
I’ve told this story several times, so if you’ve heard it, feel free to skip down a little farther. If not, here’s a little background:
I had been wearing an insulin pump for about a year by this point, and my diabetes management was okay, though I really had troubles with highs and lows. The averages were good, the peaks and valleys were not.
After we listened to the interview, the conversation went something like this:
Maureen: ”Isn’t that exciting??? I mean, isn’t that really groundbreaking?”
Me: ”Yeah, well, if they could get it to work, it would be exciting. There’s a long way between here and there.”
Maureen: ”I can’t believe you’re not excited about this. You love this stuff!”
Me: ”Okay, it’s interesting. If it works. What do you want me to do about it?”
Maureen: ”Find out about it! Someone has to be writing about it… find a blog!”
The next morning, I googled “Diabetes Blogs” and found the Diabetes Online Community.
Since then, I’ve seen countless talks and presentations and read position statements and FDA guidance on the subject. I’ve seen a lot of the work that was done at the University of Virginia on the subject.
I attended early Children With Diabetes Focus on Technology events where prototypes of the Bionic Pancreas (as it was known then) were displayed and talked about. I’ve been to FDA public workshops where evidence was presented that shows time in range for blood glucose is better than the simple A1c, and backed up with clinical data on closed loop systems.
I’ve seen the likes of Dana Lewis and Tidepool’s Howard Look speak about DIY closed loop systems, part of the #WeAreNotWaiting movement that has really helped accelerate the pace of development.
I’ve watched as now, finally, every insulin pump manufacturer in America has undertaken ongoing work to bring the best of this game-changing technology to people living with diabetes.
Through it all, I’m amazed at the dedication of the hundreds of individuals who have kept this dream alive through research, and through participation in clinical trials, pushing forward, clearing hurdle after hurdle. #WeAreNotWaiting? How about #WeAreNotGivingUp?
Recently, I’ve also thought about how much of an honor it has been, and what good fortune it has been, for me to witness this time. Access issues aside, we are all so lucky to be around during this defining moment in diabetes history.
There are so many interviews I’ve done, so many questions asked, of those working on this. But I wonder if the best interviews, the best questions, the best answers, might come a few years down the line, after closed loop insulin delivery becomes de rigueur. What stories these pioneers can tell!
In the meantime, I’ll be watching and waiting, and cheering the men and women who are changing what diabetes management looks like for this generation and beyond.