This is one in a series of posts detailing my participation in a clinical trial with an artificial pancreas element. I’m writing about this to chronicle my experience, and because if I were reading, I’d want to know about every aspect of what was going on. For more on this clinical trial, click here and here.
Last week were the final two days of my clinical trial in Virginia. This week we went through everything we went through the previous week, and everything at the same time as last week. So if I ate breakfast at 7:00 a.m. the first week, breakfast the second week was at 7:00 a.m. And it was the same breakfast. Everything, food, exercise, the whole thing, exactly like the previous week. The real difference is that in the first week, the algorithm running my artificial pancreas system was based on the data collection week I had gone through earlier in the trial. The second week, the algorithm was based on my own pump settings. The idea was to compare the special (or experimental) algorithm with something based on what I work with every day. Note: I believe this explanation is different from what I had written before. Sorry about that. Sometimes I don’t get a complete, exact idea of what is transpiring until it transpires.
I have no idea how everything turned out. Which algorithm worked better? I don’t know. And I don’t care. Because what worked best doesn’t matter. Gathering data is what matters in a trial like this. Like an A1c, the scientists working on this artificial pancreas solution need data to help them decide how to improve the device going forward. Good or bad? There is no bad data.

What was it like being hooked up to an artificial pancreas device twice in two weeks? It was… interesting. It wasn’t as “set it and forget it” as I had convinced myself it would be. And that’s one of the takeaways from this trial that really hit home for me. No matter how my external organ will perform for me in the future, I will still need to be an active participant in managing my diabetes. It’s just that an AP device would make things easier, in theory, while providing me extra protection from dangerous lows, particularly overnight.
The other big takeaway for me has to do with how an AP system is designed to work. The idea of small micro-boluses every five minutes sounds great, until your glucose starts to get up into the 200 mg/dL range. When I see a number like that a few hours after a meal, I immediately want to perform a correction bolus. A full correction, to get my BG down to the 100 mg/dL target. So in my case, if my number was 220, I would bolus three units of insulin to bring me back down to 100.

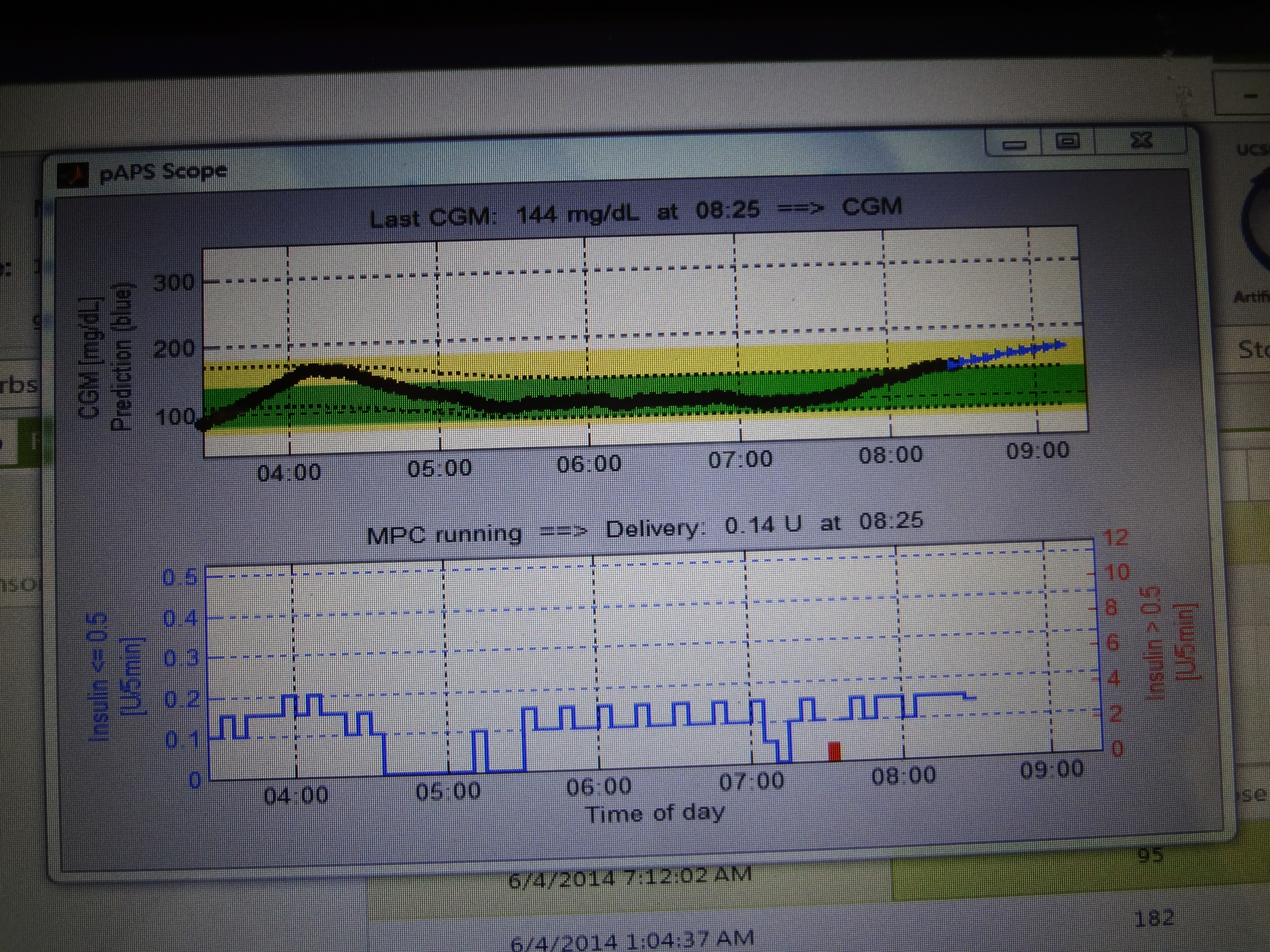
But an artificial pancreas doesn’t work that way. First of all, instead of trying to correct that number to exactly 100, maybe it would try to correct that number to a range instead. That might require a different amount of insulin. Also, my device was not going to administer all that insulin at once. It’s still going to give me small amounts, every five minutes, until I softly land in a good range (for this study, that was between 80 and 140). I think the largest amount I was given at any time (other than meals) was 0.25 units. When you look at your CGM graph on the artificial pancreas, you’ll see gentle rolling hills, instead of high mountains and deep valleys. I love the thought of that. But for me, not attacking a higher number immediately will take some getting used to. Really, it will require a completely different way of looking at my diabetes.
So in the final analysis, scientists learned something from this clinical trial (I hope), and I think I learned a lot too. When an artificial pancreas device actually hits the market at some point, I’ll be viewing it through an entirely different lens. And that’s okay. Because the older I get, the more I realize that I’m not perfect, and opening myself up to different ways to manage my disease could possibly lead to something great in the future.
——————————————————————————
Here once again is my push for clinical trial participation. Clinical trials meet a very necessary need when it comes to developing drugs, devices, and therapies that will help all People With Diabetes lead better lives. I strongly encourage you to think about volunteering for a clinical trial.
The USA’s National Institutes of Health has a complete list of clinical trials taking place all over the USA, and even some outside of my country. To find them, go to www.clinicaltrials.gov and enter “diabetes” into the search box. A recent search found 11,175 studies.
In the United Kingdom, the UK Clinical Trials Gateway is a great resource for finding out about trials happening all over Europe. To perform a search and find out more, go to http://www.ukctg.nihr.ac.uk
JDRF has a very helpful web page that lists multiple sources for registering and finding out about clinical trials. Just go to www.jdrf.org/research/clinical-trials/ to find out more.
To read more about the University of Virginia’s Center for Diabetes Technology, including staff bios and more on Artificial Pancreas technology, visit the center’s website at www.medicine.virginia.edu/research/institutes-and-programs/cdt/the-center-for-diabetes-technology-at-uva.html